A Shaky New Age
Researchers see a rocky path from genomics research to truly personalized medicines
By

Chemical & Engineering News
News last month that Illumina, a genome-sequencing technology
firm, had gotten the price of sequencing the full human genome down to
$1,000 was hailed as a great leap forward for drug research. Low-cost
sequencing is considered crucial to the medical breakthroughs promised
by the initial decoding of the human genome in 2000. Such breakthroughs
are already occurring in cancer research and elsewhere in the form of
targeted therapies—drugs designed to work on patients with specific
genetic attributes.
The drive for cures tailored to an individual patient’s biology,
known as personalized medicine, also relies heavily on genomics
research. Technological advances and successes with new drugs have bred
optimism among drugmakers and regulators that the world has entered a
new age in medical research.
“I am here to declare victory, the coming of age of this vision, this technology,” Janet Woodcock, head of the Food & Drug Administration’s
Center for Drug Evaluation & Research, told attendees at an event
sponsored by the Personalized Medicine Coalition last May. “Targeted
therapies have reached the mainstream.”
Many industry watchers, however, believe it is way too early in the
game to be declaring anything like victory. Despite the growing number
of drugs known to work with subsets of patients, critics see little
headway on the ultimate vision of tailoring therapies to individual
patients. Drug discovery efforts, they say, have been too narrowly
focused on genomics, without enough regard for the patient
information—phenotypic data—that informs about environmental influences.
The process of moving personalized therapies from the discovery lab
to the clinic is even more problematic; some observers describe it as a
disaster. The traditional method of enrolling large numbers of patients
in trials is mismatched, they say, to the mechanics of genomics-based
medical research. Meanwhile, insurance companies say they are entirely
at sea when it comes to determining how diagnostic tests that support
targeted therapies are to be reimbursed.

Woodcock
Credit: FDA
The level of frustration in some quarters is stoked by the
slow uptake of digital devices that can monitor patient health from
afar. Smartphones and other devices are capable of supplying reams of
immediately useful data on patients, providing much-needed context to
the far-more-confusing reams of genomics data on hand, according to
Bernard H. Munos, founder of the InnoThink Center for Research in
Biomedical Innovation.
“There has been a sort of disappointment in the speed with which this
whole thing is moving forward,” says Munos, a former R&D strategy
adviser at Eli Lilly & Co. In recent years, he says, researchers
have uncovered a far greater interaction between the genome and the
environment than had been assumed when genomics launched in drug
laboratories more than 15 years ago. “I don’t think we can have
personalized medicine without a lot more data about the patients
themselves,” Munos says.
Lacking these data, researchers have no access to a patient’s
presymptomatic history and other information that provide context for
genomic data. The emergence of biosensors, telemetry, and cloud
computing, according to Munos, has created a means of gathering,
storing, and transmitting data that is useful when a patient is
diagnosed with a disease. “We can access those data, play them in
reverse, and start seeing where things got off track,” he says.
George Poste, codirector of the Complex Adaptive Systems Initiative
(CASI), an effort at Arizona State University to develop
interdisciplinary research in health care, sees the work in genomics
moving toward what he calls “precision” medicine—the development of
therapies targeting patient subsets—rather than the individual patient
focus implied by personalized medicine.
Poste is concerned about the absence of phenotypic data in clinical
research and, like Munos, advocates greater use of digital technology
for monitoring patients and collecting health information. He is also
critical of the lack of standards for developing biomarkers, which are
traceable substances used to measure a biological state, and the
widespread failure to get diagnostics into the clinic. He cites critical
disconnects along the way from drug discovery to the marketplace.
“We have this asynchrony between complex science, increasing
regulatory oversight, and reimbursement,” he says. Much of the problem
centers on how data are managed at the beginning of the trek. “We have
poorly curated data from research, incompatible data sets,
interoperability problems just in the discovery arena,” he says. “How do
you migrate that into the system that you use in clinical trials? How
do you integrate that with the health care payment system?”
Sources across the spectrum from drug discovery to reimbursement
recognize dysfunction in the translation of genomics research to
approved drugs. “I would represent the ultimately frustrated person in
this regard,” says Anna D. Barker, president of the National Biomarker
Development Alliance (NBDA), which was launched last month.
Barker, who is Poste’s codirector at CASI, questions the basis for
deciding which biomarkers to pursue in drug discovery. “A lot of
biomarkers have no real clinical utility, but they are interesting
biologically,” she says. “If you ask a good clinical question and your
interest is in the clinical utility, then you have thought much
differently than someone that has just gone on a discovery exploratory
journey.”
NBDA,
whose members include drug companies, research organizations, and
patient groups, wants to develop better standards for establishing
biomarkers in an “end-to-end” system encompassing research and clinical
development, according to Barker. This will require researchers to lift
their heads from the genome, she says.
“It’s about having deep phenotypic data on patients,” she says. “That
has been a loss in this whole odyssey we have been going through in
genomics.”
NBDA will use the research enterprise’s 15 years of work on
biomarkers in establishing standards—“It’s not like we haven’t been
thinking about this stuff,” she says—while keeping an eye out for gaps
in the science. The key will be having enough of the right kind of data.
“Just having people’s genomes is not enough,” Barker says.
Tomasz Sablinski is a former Novartis researcher who left the drug company in 2008. In 2010, he launched Transparency Life Sciences,
a drug development firm. Sablinski is also unhappy with how genomics is
advancing into the clinic. “It’s a catastrophic failure,” he says. He
describes genomics as purely academic unless it translates to benefit
for patients.
And he sees a fundamental disconnect between research and the clinic.
“All of this genomics has advanced pretty much at the same speed as the
rest of the world in technology advances—cheaper, faster, more robust,”
Sablinski says. “At the same time, clinical trials are done in exactly
the same way as they were in the ’80s … in the ’60s if you stretch it.”

The clinical model that Transparency favors leverages digital devices that connect patients to clinics and data to researchers, Sablinski says. “We saw an opportunity to move things into the 21st century—a crowdsourcing idea.”
Transparency is currently using its approach to clinical trials in a
pilot study with Genentech in the area of inflammatory bowel disease.
It’s also partnering with researchers at the Icahn School of Medicine at
Mount Sinai to assess the use of metformin, a widely used diabetes
drug, to treat prostate cancer. The firm, working in partnership with
Stanford University, recently received clearance from FDA to begin Phase
IIb trials of lisinopril, a blood pressure medicine, as a treatment for
multiple sclerosis.
If clinical trials lag the science of personalized medicine, the
protocol for health care reimbursement may be even further behind.
Insurance firms are unable to determine which diagnostic tests are
covered or even ascertain which have been given, according to Michael
Kolodziej, director of oncology strategy at the insurance giant Aetna.
“The truth is that what we are doing right now is mostly getting
internal content experts together to set up ideas as to how we should
evaluate and potentially modify our current evidentiary process, because
that drives coverage,” Kolodziej says. “The problem is that the rate of
change in personalized medicine is so fast that we are questioning
whether or not we need to have another route of evaluation.”
Reimbursement for molecular diagnostics—tests that use biomarkers to
monitor disease or detect risk—poses a problem because the insurance
industry doesn’t know how to evaluate them, he says. “It would be great
if we had proficiency testing,” Kolodziej says. “Traditionally, if a
doctor orders a test, he can presume the test is done right.
Unfortunately, I don’t think we can say that’s necessarily true today in
the era of molecular testing. We honestly don’t know what people are
doing.”
Insurers say they require guidance from regulators on the analytical
validity of diagnostic tests. The insurers were completely without
guidelines prior to January 2013 when the American Medical Association
issued a standard code for some molecular diagnostic tests. “That was a
step in the right direction, but the rate of change is so fast that the
codes cannot keep up with the technology,” Kolodziej says. In the era of
next-generation sequencing, multiple tests will be run on the same
sample. There are no codes for multiple testing, he says.
The problem has been noted by the National Institutes of Health,
which is funding a study on reimbursement options for molecular
diagnostics. “But they’re projecting results for 2017,” Kolodziej says;
“2017 is infinity in this space.”
FDA’s Woodcock recognizes that the research continuum from
personalized medicine discovery to patient is still far from optimal,
but she is bemused by the contention by some that a reset button needs
to be pressed. “Different people have different ideas of what
personalized medicine is,” she tells C&EN.
With FDA’s help, momentum is building for targeted therapies,
according to Woodcock. “We clearly designated a large number of
breakthrough therapies; most of them are targeted. We are approving a
large number of targeted drugs to specific genetic defects.”
Woodcock says FDA is working with clinical data experts from the
pharmaceutical industry and the information technology sector to develop
standards for trials tailored to targeted therapies as part of the
Coalition for Accelerating Standards & Therapies, which was launched
in 2012.

Beckman
Credit: Novartis
“We are going disease-by-disease to get to outcome measures,”
Woodcock says. The group is working to coordinate standards for
established methods of collecting information and those being developed
for electronic medical records. “The goal is to do the research in the
process of an ordinary health care encounter,” she says. “But I can tell
you we are not there yet.”
Woodcock says the success of targeted therapies for cancer is proof
that personalized medicine is gaining traction. Many observers note that
most of the approved targeted drugs are for cancer, a therapeutic area
that lends itself to genomic research. Woodcock, though, points to
Kalydeco, a cystic fibrosis drug approved in 2012, as an example of a
gene-targeting therapy in an area of unmet medical need other than
cancer.
She also recognizes that some diseases will be tougher to crack with
genomics. “If you want to talk about hypertension, schizophrenia, or
diabetes, and you want to find the gene that causes that, well good
luck.”

Vincent
Credit: Pfizer
Pharmaceutical companies that have had targeted drugs approved agree
with Woodcock that the era of personalized medicine has arrived. At
Novartis, success with targeted drugs such as Ilaris, an arthritis drug,
and Afinitor, a breast cancer treatment, validates a risky change in
course that counts as a first foray by a drug firm into personalized
medicine.
Meanwhile, Novartis’s BYM338, a monoclonal antibody in development as
a targeted therapy for sporadic inclusion body myositis, has been
awarded breakthrough status by FDA, as has its breast cancer drug
candidate LDK378, for which the company has filed for registration
following Phase II trials.
“The notion of looking at pathways and homogenous patient subsets
before broad populations is something we try to do in every program.
That’s our mantra,” says Evan Beckman, head of translational medicine at
the Novartis Institutes for BioMedical Research (NIBR), adding that
advances in genome screening have fed breakthroughs at Novartis. “These
technologies have enabled the whole NIBR mission.”
Beckman says he is bullish regarding the progress of personalized
medicine, but he is not surprised at the frustration expressed by
others. “Any biological revolution gets translated into hype very
quickly, and the real work takes work,” he says. “To me, we are really
emerging into a golden age.”
Novartis has not had difficulty advancing basic research into the
clinic, Beckman claims, because of NIBR’s strategy of assigning
physician-scientists to research projects from their inception. By
anticipating at the test-tube and animal-test stages what will be
required at the first-in-human stage, the company is able to compile the
most pertinent preclinical data to design effective trials.
The first fruits have been in oncology, he acknowledges, and
personalized medicine continues to struggle for a foothold elsewhere.
“Probably the most important limitation that has befallen the general
medicine piece is matching the genetic DNA with a good phenotype of the
patient,” he says.
Michael S. Vincent, vice president of biotherapeutic clinical R&D at Pfizer,
is less sanguine about the new age of targeted therapies, acknowledging
that proteomics and other “omics” technologies fell short of
expectations. Some were even discredited. He now sees researchers
navigating a structural gap between genomics-based target selection and
the traditional clinical protocol.
“Whenever you start incorporating a data-dense information stream,
the traditional clinical infrastructure kind of breaks down,” Vincent
says. Next-generation sequencing data and clinical data have to be made
to mix, however. Pfizer has established a separate pipeline to work with
exploratory data, unburdening the process from a strict clinical
protocol, according to Vincent. Thus sequestered, the data are
interrogated to identify the analytes that make sense to develop in a
way that he says will eventually pass regulatory muster
.
.
“The focus is on the science,” he says. “You may not have a strong
hypothesis going in, but you are going to collect enough data so that
you may be able to make a robust inference at the end. There is no shame
in doing hypothesis-free science.”
Eric Topol, director of Scripps Translational Science Institute,
agrees with Novartis’s Beckman that any revolutionary change in
medicine takes a long time to fold into the system. He points out that a
great deal of human biology was not taken into consideration in the
early days of genomics research.
“In recent years there has been marked appreciation of the gut
microbiome,” Topol says. “I don’t think anybody back in 2003 had any
idea how important that could be in regard to our immune system and our
susceptibility to everything from obesity to diabetes to autoimmune
disorders to cancer.” The impact of the epigenome and the human
methylome on disease is also now appreciated.
“There is this whole parallel path of heritability that isn’t DNA
dependent,” he says. “Finally, I don’t think that back then people knew
we would have sensors that would measure any physiologic metric of man
with a smartphone. And when you start doing that and start looking at
somebody’s physiology in real time, you say, ‘Whoa, there is a lot of
information there that you can’t get out of the DNA sequencing or other
‘omics.’ ”
Topol says he is more frustrated by what the clinical research
community does know but hasn’t acted upon.
“There is an incredible amount of knowledge about individualized treatments that we are not using,” he says. “I’m talking about drugs that are out there that are some of the most commonly used drugs where we know the particular genomic variant that predicts horrendous side effects or efficacy, and we don’t even use that information. It’s pathetic.”
“There is an incredible amount of knowledge about individualized treatments that we are not using,” he says. “I’m talking about drugs that are out there that are some of the most commonly used drugs where we know the particular genomic variant that predicts horrendous side effects or efficacy, and we don’t even use that information. It’s pathetic.”
He cites Tegretol, a neuropsychiatric therapy with potentially fatal
dermatological reactions that in other countries is prescribed only
after simple genotype safety testing. “Here in the U.S., we don’t test
for it. We play Russian roulette, basically,” he says.
Similarly, Topol is critical of the pharmaceutical industry
for not pushing forward on screening to find target populations for
best-selling biologic drugs such as Humira, Remicade, and Enbrel. “These
drugs have a collective $30 billion in sales per year and maybe at best
a 30% clinical response rate,” he says. “Why are we not going
full-court press on finding out who responds and who doesn’t, so we
don’t waste $18 billion to $20 billion a year?”
Doing so would likely require more specialized testing, such as
immune repertoire sequencing and antibody sequencing, in addition to
genome sequencing, “but there are not enough aggressive attempts to go
after it,” he says.
Several critics decry an innate intransigence in the health care industry that is working against personalized medicine.
Munos at InnoThink points to huge savings that can be reaped by bringing clinical trials in line with modern digital technology. But doing so would likely meet with resistance among hospitals that stand to lose significant revenue if trials were crowdsourced.
“Let’s face it, many people in different organizations make a very
comfortable living out of this dysfunctional state of affairs,” Munos
says. Health care, he adds, will not easily be reformed, but it will be
disrupted by technologies that create new access to data from patients.
The system will be forced to change.
Pfizer’s Vincent notes that the traditional training of researchers
will also be disrupted. “We’ve got a new breed of computational
biologists that didn’t exist 15 years ago, and you need clinicians and
clinical scientists who know how to talk to those people,” he says.
“What is needed are people who have a multidisciplinary training, who
can understand the clinical, medical, pathophysiological, and
pharmacological bases of the disease and the patient—and turn them into
something meaningful.”
Meaning, according to Poste at Arizona State, is defined by the
patient, and the patient, in turn, is defined by data. “In the end,”
Poste says, “everything we generate, irrespective of which technologies
we use, should give rise to robust information that enables better
clinical decisions and cost control.”
- Chemical & Engineering News
- ISSN 0009-2347
- Copyright © 2016 American Chemical Society
Psychedelic compounds like ecstasy may be good for more than just a high
Scientists are testing whether drugs that alter consciousness can treat intractable mental health conditions
By

Credit: Yang H. Ku/C&EN/Shutterstock
In brief
Conventional psychiatric and other therapies often fail to help
people with mental health conditions. Some researchers are now turning
to promising treatments from the 1950s and 1960s: psychedelic compounds
that were largely banned in the 1970s as reaction to cultural and
political turmoil linked to recreational drug use. Here, C&EN
examines how ibogaine, MDMA, marijuana, ketamine, and psilocybin might
be used clinically.

Credit: Yang H. Ku/C&EN/Shutterstock
While studying alkaloid natural products and their derivatives, Sandoz chemist Albert Hofmann
had to leave the lab early one day in 1943 because he’d accidentally
been exposed to one of his products, lysergic acid diethylamide (LSD).
As he wrote in his memoir, “LSD—My Problem Child,”
he later reported to his department director: “I was forced to
interrupt my work in the laboratory in the middle of the afternoon and
proceed home, being affected by a remarkable restlessness, combined with
a slight dizziness. At home I lay down and sank into a not unpleasant
intoxicated-like condition, characterized by an extremely stimulated
imagination. In a dreamlike state, with eyes closed … I perceived an
uninterrupted stream of fantastic pictures, extraordinary shapes with
intense, kaleidoscopic play of colors. After some two hours this
condition faded away.”
In the decades that followed, various researchers pursued LSD and
other psychoactive compounds for medical uses, looking to use them to
treat mental health disorders such as schizophrenia and depression.
Then the 1960s arrived, with the baby boom generation embracing an
antiestablishment ethos as well as recreational drug use. Governments
responded, in part, with the 1971 Convention on Psychotropic Substances,
a United Nations treaty that led to bans on psychedelic compounds. “It
was a reaction to cultural and political turmoil that was thought to be
in some way tied in with youth culture getting involved in
psychedelics,” says Charles Grob,
a professor of psychiatry and pediatrics at the University of
California, Los Angeles, School of Medicine and chief of child and
adolescent psychiatry at Harbor-UCLA Medical Center. Contrary to
scientific findings, the compounds were branded as having no medical use
and a high potential for abuse.
Now, however, as clinicians find that conventional treatments for
mental health conditions fail many patients, Grob and others have
resumed research on psychedelics despite the barriers. With depression,
for example, “there are some people that respond well to standard
antidepressant medications but a lot of people who don’t, even through
many trials of different medications and combinations of them,” says David Feifel, a professor of psychiatry at the University of California, San Diego. “There’s a big need for something more.”
Feifel and other scientists are looking for that “something more” in
compounds such as ibogaine, MDMA, ketamine, and psilocybin (the
psychoactive ingredient in magic mushrooms). Researchers are also
investigating beneficial uses for marijuana and its natural
cannabinoids. Potential applications include treating addiction,
posttraumatic stress disorder, neuropathic pain, epilepsy, and anxiety
caused by diagnosis of a life-threatening illness such as cancer.
Research into using these compounds as medicines is in early stages,
and the legal environment surrounding them makes studies difficult to
conduct. U.S. researchers and their suppliers must obtain a special license from the Drug Enforcement Administration.
Licensing requirements might include storing a drug supply in a safe
that’s inside a room equipped with alarms, plus careful record keeping
as compounds are dispensed to ensure none has gone missing.
Obtaining funding for clinical studies of psychedelics is also
challenging. Pharmaceutical companies are generally uninterested in
pursuing the compounds because their potential uses are already
well-known, limiting companies’ ability to patent them and gain market
exclusivity, says Rick Doblin, founder and executive director of the Multidisciplinary Association for Psychedelic Studies
(MAPS), which finances clinical trials. Donors to MAPS, which has a
$3.5 million budget this year, include the social justice organizations Libra Foundation and RiverStyx Foundation, cleaning and personal care product manufacturer Dr. Bronner’s, the online community Reddit, and “aging baby boomers and tech millionaires,” Doblin says.
Then there is the societal concern that making psychedelic compounds
available as pharmaceuticals will increase drug addiction and abuse. “I
understand the concerns, but most classic psychedelics, such as
psilocybin, don’t fit the conventional profile of a drug of abuse,” says
Roland R. Griffiths,
a professor of psychiatry and behavioral sciences at Johns Hopkins
University. He has spent most of his career funded by the National
Institute on Drug Abuse to study psychoactive compounds and the
properties that make them addictive. He is also now running clinical
trials using psilocybin to treat anxiety and depression in cancer
patients.
The pharmacology of many psychedelics is different from opiates,
which are highly addictive. People build up a tolerance to psychedelics
that can’t be overcome with a higher dose, and they also don’t show
withdrawal symptoms. What’s more, Griffiths says, the altered
consciousness of a psychedelic trip can be “fantastically interesting”
but also psychologically difficult to handle and unpredictable. He and
others say that although their patients appreciate the psychedelic
experiences, people don’t typically ask for more doses than necessary.
Some of Feifel’s patients even postpone a repeat dose if they’re still
doing well after the previous one.
As for adverse events, those are rare for pure drug material such as
that used in clinical trials, researchers say. Negative reactions
typically happen when people use recreational products that have been
adulterated by questionable sellers.
That’s not to say that psychedelics are perfectly safe. As with all
approved or potential pharmaceuticals, “we’re dealing with a
cost-benefit analysis,” says Igor Grant, a professor of psychiatry at
the University of California, San Diego, and director of California’s
Center for Medicinal Cannabis Research. “No drug is harmless. We need to
really establish from a medical standpoint what the uses and
limitations are.”
The following are several compounds being studied.

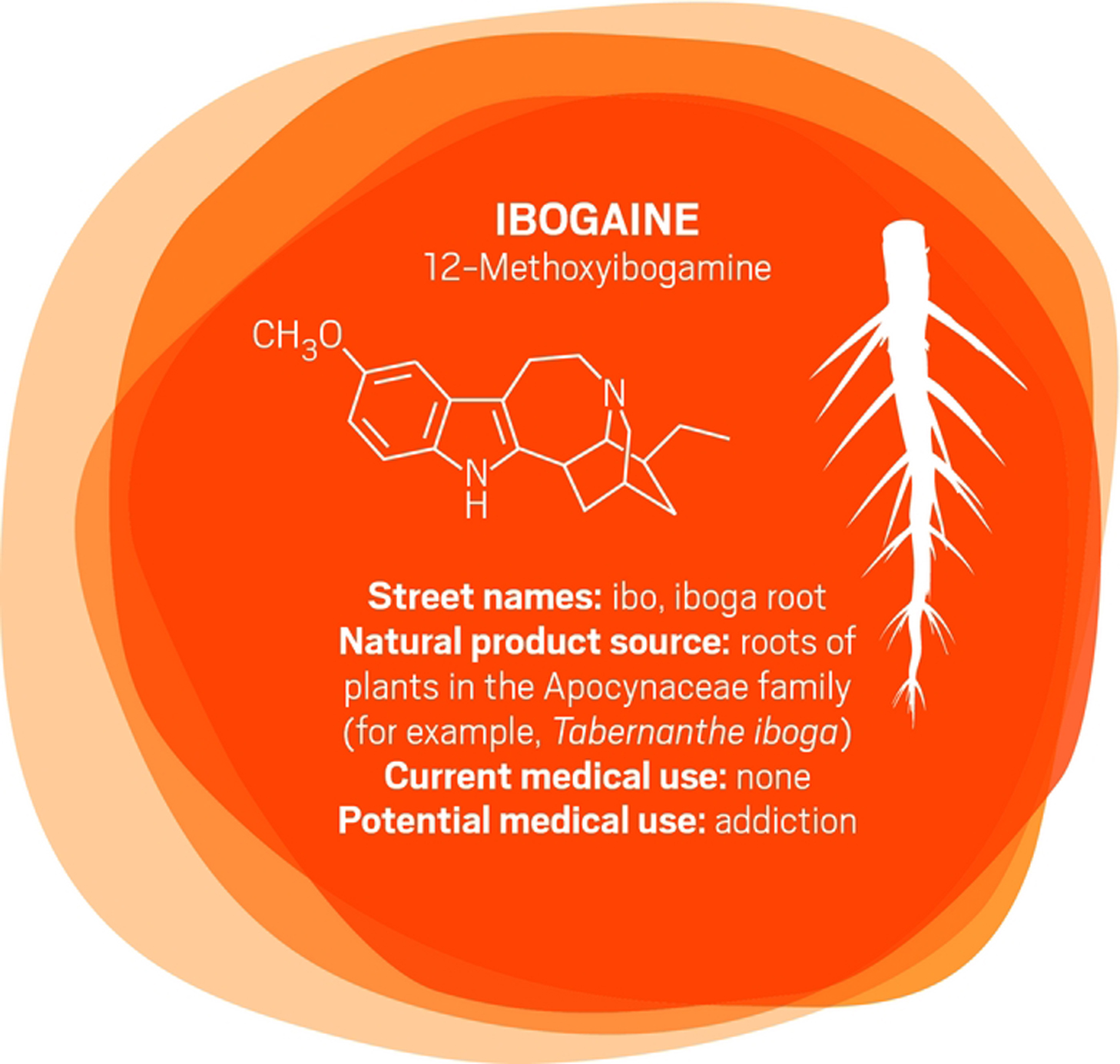
In the early 1990s, University of Miami neurology professor Deborah C. Mash traveled to Amsterdam to see ibogaine
treatments firsthand. “A single dose of ibogaine could completely block
the signs and symptoms of opiate withdrawal,” says Mash, who has spent
her career studying the effects of drugs and alcohol on the brain. She
and others are now studying ibogaine as a treatment for opiate, cocaine,
alcohol, and nicotine addiction.
Ibogaine was first isolated in 1901. It interacts with glutamate
receptors in the brain that are involved in learning, memory, and
creation of new neural pathways. The receptor interactions are likely
the source of ibogaine’s consciousness-altering effects.
But ibogaine is metabolized within 24 hours: A hydroxyl replaces
ibogaine’s methoxy group, producing noribogaine. Noribogaine binds to
serotonin transporter, opioid, and nicotinic receptors and is cleared
from the body slowly. Consequently, noribogaine is likely the compound
that’s responsible for reducing patients’ withdrawal symptoms and
cravings over the long term, as well as the accompanying anxiety and
depression (Neuropharmacology 2015, DOI: 10.1016/j.neuropharm.2015.08.032).
Mash has patented noribogaine and related compounds, as well as their
formulations. She founded a company, DemeRx, to bring them into
clinical treatment. DemeRx is currently running a Phase II clinical
trial to evaluate noribogaine’s use as an alternative to methadone or
Suboxone to help opioid addicts transition to sobriety in combination
with support for behavioral changes.
Even if the noribogaine trials are successful, ibogaine could still
have a role in addiction treatment because the “waking dream” experience
it offers seems to help patients as well. “We work with people who have
been hard-core addicts, abusing drugs and alcohol for more than a
decade,” Mash says. As with other psychedelics, ibogaine induces an
experience that patients report helps them gain insight into their
destructive behaviors. That new awareness helps them be more open to
therapy and lifestyle changes. “A combination protocol of a dose of
ibogaine followed by noribogaine for maintenance could be optimal,” Mash
says, “although more work is needed to determine whether that is the
best approach.”

“After 100 years of modern psychiatry, our current best treatment for
trauma-related disorders is only effective for 50% of people,” says
U.K. psychiatrist Ben Sessa.
The cure for posttraumatic stress disorder (PTSD) is
psychotherapy—talking through and processing the trauma with a mental
health specialist. “About half of people will talk and, over weeks or
months, will overcome their high level of distress and get better,”
Sessa says. For others, talking about their experience is overwhelming.
“They drop out of treatment and use dangerous drugs such as alcohol to
mask their symptoms. They have high levels of self-harm and high levels
of completed suicide,” Sessa says.
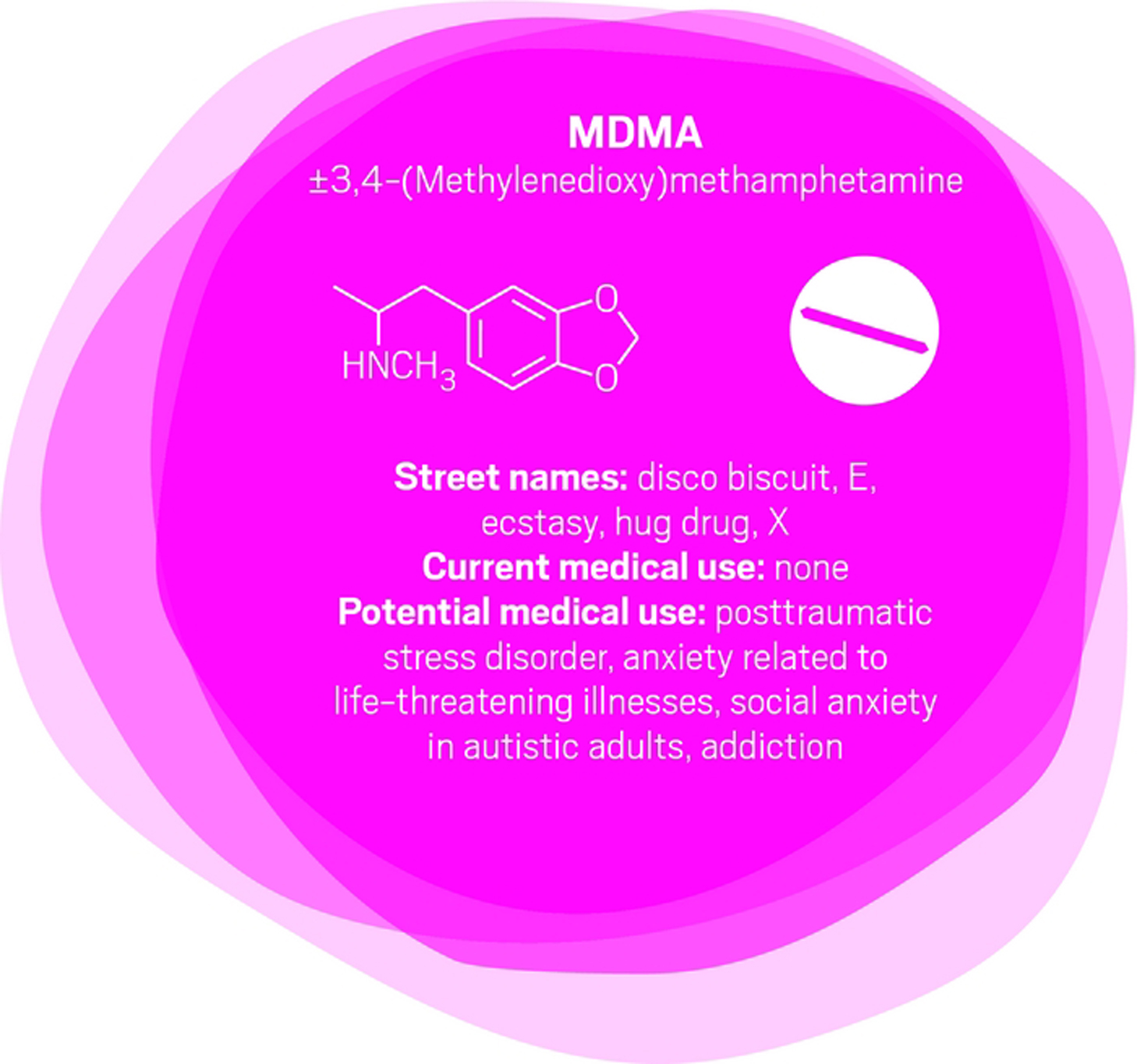
MDMA
interacts with a transporter in the brain that causes the release of
serotonin, which in turn causes the release of other neurotransmitters
and hormones. For people who might otherwise flee psychotherapy, MDMA
reduces fear and increases trust and empathy. MDMA is also mildly
stimulating rather than sedating. The overall effect is to calm patients
and help them engage with a therapist about difficult experiences.
Sessa likens MDMA to a life jacket.
U.S. psychiatrist Michael Mithoefer
leads clinical trials studying MDMA for PTSD. In an initial trial,
Mithoefer and colleagues worked with patients who had PTSD for an
average of 20 years, mostly from sexual trauma. The patients had
undergone previous psychotherapy for an average of almost five years and
were not helped by conventional antidepressants. They received MDMA or a
placebo two to three times, with doses one month apart, as part of
eight-hour sessions with two therapists followed by an overnight stay at
the clinic for continued monitoring (J. Psychopharmacol. 2010, DOI: 10.1177/0269881110378371).
Going through the psychedelic experience, patients could focus inward
and stay quiet as they wished or talk with the therapists. They also
had extensive preparatory and follow-up psychotherapy sessions. Of 12
patients who received MDMA, 10 of them (83%) showed significant relief
of their PTSD symptoms. In the placebo group, only two out of eight
patients (25%) showed improvement with the same psychotherapy support.
Other studies
show similar positive results, although “it is hard to have an
effective ‘blind’ with this type of substance,” Mithoefer concedes,
because patients can usually tell whether they’ve been given a placebo
or the real thing.
Nevertheless, the Multidisciplinary Association for Psychedelic
Studies aims to start Phase III trials for PTSD next year, with MDMA
synthesized by an unnamed U.K. contract manufacturing company following
current Good Manufacturing Practices.

“There is a very, very broad range of medical conditions for which cannabis or its constituent chemicals could find applications,” says Daniele Piomelli,
a professor of neuroscience and pharmacology at the University of
California, Irvine. However, few good clinical studies have been
completed.
Mammals naturally make some cannabinoids, including anandamide, which
likely plays a role in stress response and social behavior, and
2-arachidonoylglycerol, which is involved in modulating activity at the
brain’s nerve cell junctions.
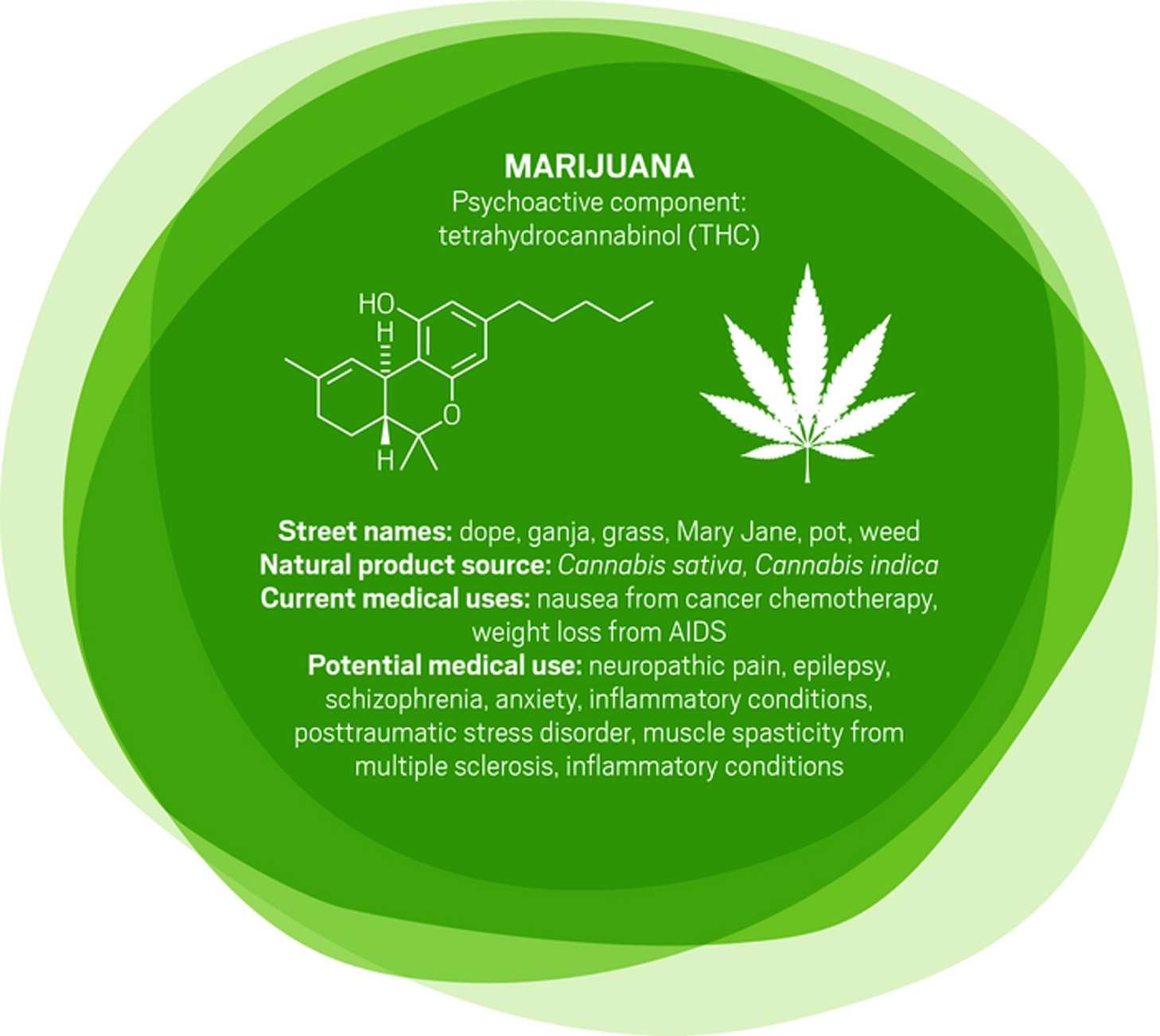
Other cannabinoids, such as those produced in marijuana, can target the same neurological receptors as endogenous cannabinoids. Tetrahydrocannabinol is the one that generates a psychoactive response. It is already approved as dronabinol
to treat nausea in patients undergoing cancer chemotherapy and appetite
loss in people with AIDS. “It’s a poor drug,” Piomelli says. It has
poor bioavailability and has a complex metabolism, he adds.
Researchers are studying another cannabis compound, cannabidiol,
to treat seizure disorders, schizophrenia, and other conditions.
Cannabidiol is not psychoactive, but unraveling its pharmacology is
difficult because it interacts with a variety of receptors beyond the
endocannabinoid system.
And some scientists are testing whole plant material. California’s Center for Medicinal Cannabis Research, for example, has studied smoked or vaporized cannabis to treat neuropathic pain, which originates in damaged nerve fibers (J. Pain 2015, DOI: 10.1016/j.jpain.2015.03.008). Short-term pain studies indicate that cannabis relieves the pain, “but what we haven’t answered is whether it works forever,” says Igor Grant,
director of the center and a professor of psychiatry at the University
of California, San Diego. “Does the efficacy remain, or do people get
used to it and it no longer works as well? Is it possible that after a
year you see side effects that you don’t see after a few weeks?”
With broadening legalization of medical and recreational marijuana in
the U.S., “a lot of people are self-testing for a number of different
conditions,” Piomelli says. “We typically hear about positive favorable
effects because those tend to surface, but we don’t have studies that
are done appropriately for all these different uses.”

Compared with conventional antidepressants, ketamine
is “remarkable,” says David Feifel, a professor of psychiatry and
director of a center specializing in advanced treatments for depression
at the University of California, San Diego.
Starting in 2004, Carlos A. Zarate Jr.,
chief of the Experimental Therapeutics & Pathophysiology Branch of
the National Institute of Mental Health, led a study in which his team
used ketamine to treat 17 patients who had already been through an
average of six antidepressants. They observed 12 patients (71%) improve
within 24 hours.
That speedy response time contrasts with conventional antidepressants
such as sertraline and fluoxetine, which target serotonin pathways in
the brain and typically take weeks to work.
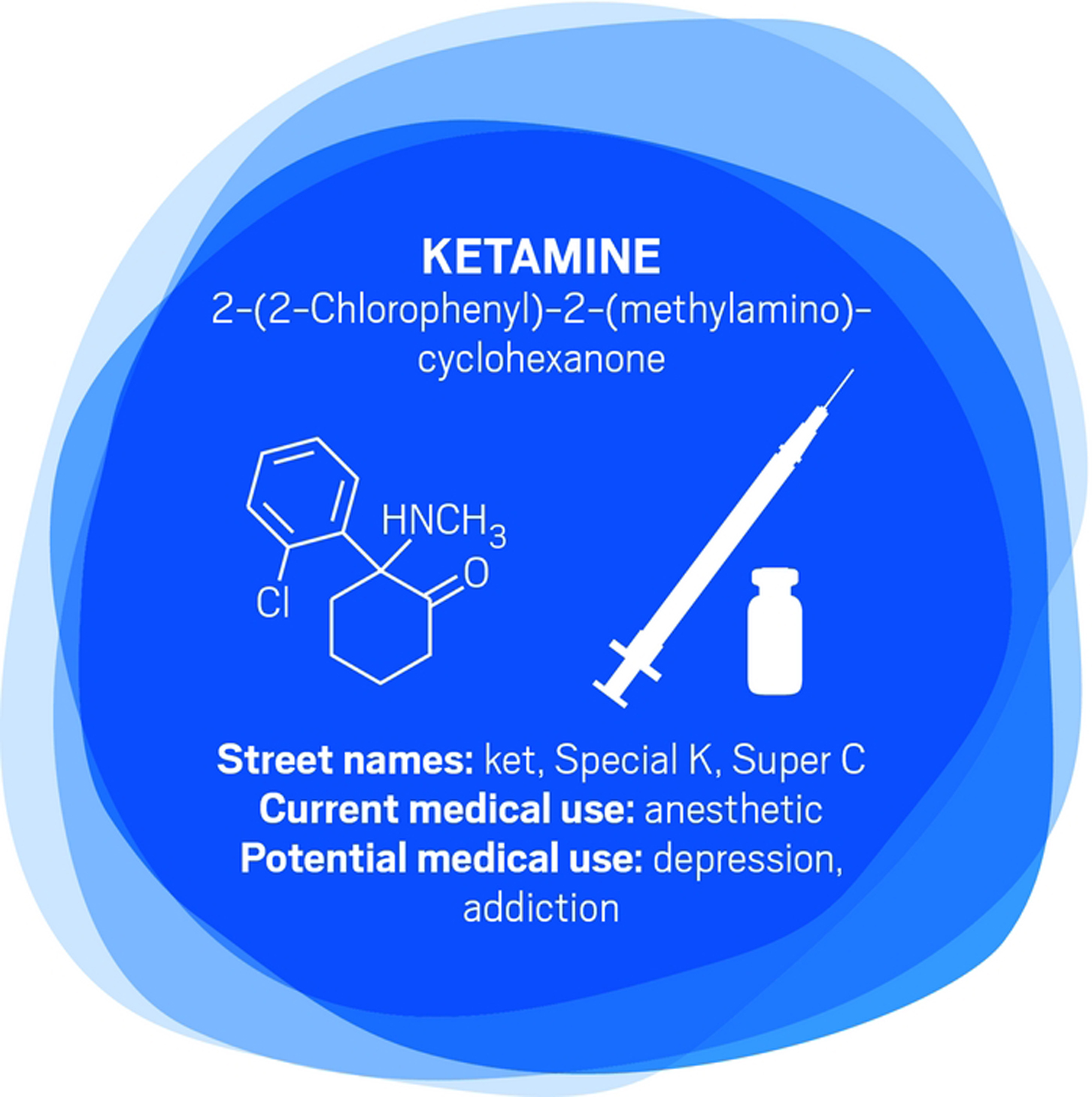
Ketamine binds to the same glutamate receptors as ibogaine. Its
half-life in the body is two to three hours. But ketamine’s relief of
depression lasts an average of around seven to 18 days, with some
patients improving for as long as five months, Feifel says.
Zarate is conducting a range of studies—including neurological
imaging, proteomics, and metabolomics—to unravel ketamine’s effects in
the brain. He points to dehydronorketamine as a particularly interesting
metabolite. Zarate and colleagues have found that it may play a role in
alleviating depression by interacting with a nicotinic receptor
involved in long-term memory (Eur. J. Pharmacol. 2013, DOI: 10.1016/j.ejphar.2012.11.023).
A racemic mixture of ketamine enantiomers is currently approved and
manufactured for use as an anesthetic. Doctors administer it for
depression off-label as an injection or intravenous infusion, at a dose
low enough to avoid unconsciousness. Johnson & Johnson’s Janssen
R&D unit has an intranasal formulation of the S-(+)-ketamine enantiomer, known as esketamine,
in clinical trials. In both cases, patients are dosed in clinics and
monitored until the altered consciousness effects dissipate. Allergan is
developing a related compound, rapastinel, that targets the same glutamate receptors but does not induce altered consciousness.
None of the compounds provides a single-dose cure for depression—they
all require continuing treatment. Nevertheless, they could be a
much-needed help for people who have otherwise lost hope. Says Feifel,
“Were it not for the ketamine treatments that they receive, it’s highly
likely that several of our patients would not be around today.”

“It was unlike anything I’ve seen in psychopharmacology before,” says
Roland R. Griffiths, a professor of psychiatry and behavioral sciences
at Johns Hopkins University, of his first trial examining the safety of
psilocybin in healthy volunteers.
Those volunteers had positive effects that could last for years.
“People had increased satisfaction and quality of life,” Griffiths says.
“They felt more generous, centered, optimistic, and caring toward other
people in their lives.” Patients’ friends, family members, and work
colleagues confirmed the differences.
Griffiths has since conducted trials of psilocybin for tobacco
addiction, anxiety, and depression in patients with life-threatening
cancer.
Like MDMA, psilocybin targets serotonin receptors. Also like MDMA,
the effects of psilocybin seem to stem from patients’ experiences when
their consciousness is altered. But instead of undergoing psychotherapy
during the acute psilocybin experience, researchers encourage patients
receiving psilocybin to focus inwardly and have a deeper experience
described as mystical or spiritual by doctors such as Griffiths.
Processing with a therapist comes later.
“The best treatment outcomes are with those subjects who, during the
course of the psilocybin session, had what they described as a profound
psychospiritual epiphany,” says Charles Grob, a professor of psychiatry
and pediatrics at the University of California, Los Angeles, School of
Medicine and chief of child and adolescent psychiatry at Harbor-UCLA
Medical Center (Arch. Gen. Psychiatry. 2011, DOI: 10.1001/archgenpsychiatry.2010.116).
Cigarette smokers given psilocybin report that the drug helps them
understand their nicotine craving. That makes them able to quit more
successfully when they’re also undergoing a cognitive behavioral therapy
program for tobacco addiction, Griffiths says (J. Psychopharmacol. 2014, DOI: 10.1177/0269881114548296).
For people diagnosed with cancer and struggling with the existential
fears associated with dying, “it’s harder to say what the nature of the
attitude shifts are,” Griffiths says. “But it seems to be an increased
sense of wonder and openness to the mystery of life and death. In spite
of the tragedy that they’re dying, they might see that there’s something
beautiful and organic about the process.”
- Chemical & Engineering News
- ISSN 0009-2347
- Copyright © 2016 American Chemical Society

{kind=link}